1-Testosterone — dihydroboldenone
1-Testosterone is an anabolic steroid that is derived from dihydrotestosterone. More specifically, it is a dihydro (5-alpha reduced) form of the anabolic steroid boldenone. It is also structurally very similar to Primobolan (methenolone), except that 1-testosterone lacks the additional 1-methyl group used to increase steroid oral bioavailability. The activity of this steroid is that of a strong anabolic agent, with moderate androgenic properties. The standard rat assays show it to be approximately twice as anabolic as testosterone propionate, while it retains a similar level of androgenicity. This gives it an anabolic ratio of about 2, which means it is twice as anabolic as it is androgenic. 1-testosterone is one of the most potent naturally occurring steroids to be isolated, and is valued by bodybuilders for its ability to promote significant muscle tissue gains without water bloat or strong side effects.
| Brand name | 1-Testosterone, Dihydroboldenone | |||
| Androgenic | 100 | |||
| Anabolic | 200 | |||
| Standard | Testosterone propionate | |||
| Chemical Names | 17beta-hydroxyandrost-1-en-3-one 5alpha-androst-1 -en-3-one,17beta-ol |
|||
| Estrogenic Activity | low | |||
| Progestational Activity | no data available |
1-Testosterone History
Although synthesized some years earlier, the first detailed mention of 1-testosterone in the Western medical literature seems to come in 1962. It was favorably studied (on a limited basis), but never developed as a prescription drug product, likely for a simple lack of financial viability (there are literally thousands of testosterone analogs that have been developed over the years, but certainly no incentive to try and develop all of them into medicines). It was once placed into development as an ether derivative (1-methoxycyclohexyloxy) called mesabolone, but even this was very short lived. 1-testosterone had essentially been lost in the steroid research books for decades, and was all but forgotten. Things changed very quickly in 2002, however, when the drug was released to the U.S. market as a nutritional supplement. Although technically questionable in a legal sense, the popularity of the new hormone was rapid and extreme, and countless OTC 1-testosterone products soon followed.
1-Testosterone is not intrinsically a very orally active hormone. Therefore, it is a little difficult to create a product of high potency with this method of administration. It is very much like taking a powerful hormone such as testosterone, and trying to stuff it in a capsule. The liver is too efficient at breaking steroids down for this to be effective. When 1-testosterone was available as a supplement in the U.S., oil-solubilized softgels using 1-testosterone tetrahydropyranyl ether, hexyldecanoate ester, and undecanoate ester were the most effective products. These products resembled Andriol, which dissolves an ester-modified form of testosterone (undecanoate) in oil to help deliver the steroid to the body via the lymphatic system (bypassing the destructive first-pass through the liver).
Some companies were also formulating this steroid in transdermal gels during this time, which is another effective method of getting this hormone into your body. These products were designed in a similar fashion as Androgel, and likely delivered about 10% of the applied dose to the body systemically. Lastly, there were a few products that were made as injectables (1-testosterone cypionate), which reportedly worked very well. This would be the preferred method of using 1-testosterone, although no legitimate prescription drug preparation like this has ever existed (these were essentially injectable drug products created by unregulated supplement companies). While many consumers used them with great success, there was simply no government oversight assuring such products were made to pharmaceutical specifications.
1-Testosterone was sold on the sports supplement market in the U.S. for approximately three years. It was finally classified as a Class III controlled substance in January 2005, as part of an expanded Anabolic Steroid Control Act that was passed by Congress that sought to eliminate OTC steroids. These products were most often described by their manufacturers as prohormones or prosteroids, although were in reality often just unscheduled (unknown to lawmakers) steroids. Given that no legitimate pharmaceutical preparation has ever contained 1-testosterorone, the passing of this law effectively marked the commercial end of this anabolic steroid. At the present time, no 1-testosterone preparations are known to exist, and the agent is once again unavailable to athletes.
How is 1-Testosterone Supplied
No prescription drug product containing 1-testosterone currently exists. It was sold as an OTC supplement in the U.S. between 2002 and 2005, produced in various oral, transdermal, and injectable forms.
Structural Characteristics of 1-Testosterone
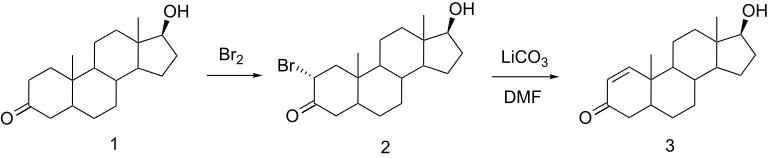
1-Testosterone is a derivative of dihydrotestosterone. It contains one additional double bond between carbons 1 and 2 (1-ene), which helps to stabilize the 3-keto group and increase the steroid’s anabolic properties.
Note that the name 1 -testosterone is actually a misnomer, and is not a formal identification for this drug. The term 1-testosterone is more appropriately applied to the steroid boldenone, which consists of a testosterone molecule modified with a 1-ene group. Given the widespread association of 1-testosterone with this steroid, however, it has been identified as such in this reference book.
1-Testosterone Side Effects (Estrogenic)
1-Testosterone does metabolize to estrogen in the body, even though there is no evidence that the body can insert a double bond at carbon-4. The exact nature of this transformation is unknown. Given experiences with the hormone, 1-testoserone is considered to be only a mild estrogenic steroid. Estrogen-linked side effects are generally not seen when administering this steroid, including gynecomastia, fat deposition, and visibly increased water retention. Gains made with 1-testosterone tend to be quality muscle mass, not the smooth bulk that often accompanies steroids highly open to aromatization. 1-Testosterone is, therefore, a steroid most favored during cutting phases of training, when water and fat retention are major concerns, and sheer mass not the central objective.
1-Testosterone Side Effects (Androgenic)
Although classified as an anabolic steroid, androgenic side effects are still possible with this substance. This may include bouts of oily skin, acne, and body/facial hair growth. Anabolic/androgenic steroids may also aggravate male pattern hair loss. Women are warned of the potential virilizing effects of anabolic/androgenic steroids. These may include a deepening of the voice, menstrual irregularities, changes in skin texture, facial hair growth, and clitoral enlargement. Due to its lower relative androgenicity, women often find this preparation an acceptable choice provided low doses are used. Although 1-testosterone is primarily anabolic in nature, strong androgenic side effects are possible with higher doses, and should be carefully monitored. Note that the 5-alpha reductase enzyme does not metabolize 1-testosterone, so its relative androgenicity is not affected by finasteride or dutasteride.
1-Testosterone Side Effects (Hepatotoxicity)
1-Testosterone is not known to be a hepatotoxic steroid; liver toxicity is unlikely within normal parameters of use. Note that studies have shown that 1-testosterone significantly increases liver weight (unlike testosterone), suggesting that risk of liver toxicity cannot be completely excluded with high doses or prolonged administration.
1-Testosterone Side Effects (Cardiovascular)
Anabolic/androgenic steroids can have deleterious effects on serum cholesterol. This includes a tendency to reduce HDL (good) cholesterol values and increase LDL (bad) cholesterol values, which may shift the HDL to LDL balance in a direction that favors greater risk of arteriosclerosis. The relative impact of an anabolic/androgenic steroid on serum lipids is dependant on the dose, route of administration (oral vs. injectable), type of steroid (aromatizable or non-aromatizable), and level of resistance to hepatic metabolism. 1-Testosterone should have a stronger negative effect on the hepatic management of cholesterol than testosterone or nandrolone due to its weakly aromatized nature, but a weaker impact than most c-17 alpha alkylated steroids. Due to the route of delivery, oral 1-testosterone will have a slightly stronger negative effect on lipids compared to injections. Anabolic/androgenic steroids may also adversely affect blood pressure and triglycerides, reduce endothelial relaxation, and support left ventricular hypertrophy, all potentially increasing the risk of cardiovascular disease and myocardial infarction.
To help reduce cardiovascular strain it is advised to maintain an active cardiovascular exercise program and minimize the intake of saturated fats, cholesterol, and simple carbohydrates at all times during active AAS administration. Supplementing with fish oils (4 grams per day) and a natural cholesterol/antioxidant formula such as Lipid Stabil or a product with comparable ingredients is also recommended.
Side Effects (Testosterone Suppression)
All anabolic/androgenic steroids when taken in doses sufficient to promote muscle gain are expected to suppress endogenous testosterone production. Without the intervention of testosterone-stimulating substances, testosterone levels should return to normal within 1-4 months of drug secession. Note that prolonged hypogonadotrophic hypogonadism can develop secondary to steroid abuse, necessitating medical intervention.
1-Testosterone Administration (General)
Note that 1-testosterone is slightly an intrinsically irritating substance. This makes injection with the base hormone, even transdermal delivery at times, uncomfortable, producing skin/tissue irritation and redness. Some users even tend to notice a burning sensation when urinating while taking any 1-testosterone product. Although poorly understood, this side effect has never been reported to be dangerous, and is generally looked at as an inconvenience among users.
1-Testosterone Administration (Men)
1-Testosterone was never approved for use in humans. Prescribing guidelines are unavailable. For physique- or performance-enhancing purposes, a daily dosage is usually in the range of 100-250 mg with oil-solubilized softgels, or 75-100 mg daily when applied as a transdermal. Injectable dosages would fall in the range of 100-200 mg per week (as 1-testosterone cypionate). The drug is typically taken in cycles of 6-12 weeks. Users of 1 -testosterone generally report lean gains in muscle mass, which are often accompanied by body fat reductions and an increased appearance of hardness to the physique.
1-Testosterone Administration (Women)
1-Testosterone was never approved for use in humans. Prescribing guidelines are unavailable. For physique- or performance-enhancing purposes, doses of 25 mg daily or less (oil solubilized softgels or transdermal) are usually used. The drug is typically taken in cycles of 4-6 weeks. Given that most preparations contained high concentrations of drug, 1-testosterone was not widely used by females.
1-Testosterone Availability
1-Testosterone is not currently produced as a prescription drug product.
References
Wlliam Llewellyn (2017) – Anabolics
Your experience with 1-Testosterone — dihydroboldenone


About Author
baxx
Doctor Baxx is an internationally recognized leader in the competitive bodybuilding industry. Its advanced bodybuilder and fitness training specialist certification provides beginners with opportunities for further advancing their knowledge and skills with bodybuilding at the advanced level.