Anadrol — oxymetholone
Oxymetholone is a potent oral anabolic steroid derived from dihydrotestosterone. More specifically, it is a close cousin of methyldihydrotestosterone (mestanolone), differing only by the addition of a 2-hydroxymethylene group. This creates a steroid with considerably different activity than mestanolone, however, such that it is very difficult to draw comparisons between the two. For starters, oxymetholone is a very potent anabolic hormone. Dihydrotestosterone and mestanolone are both very weak in this regard, owing to the fact that these molecules are not very stable in the high enzyme (3-alpha hydroxysteroid dehydrogenase) environment of muscle tissue. Oxymetholone remains highly active here instead, as is reported in standard animal assay tests demonstrating a significantly higher anabolic activity than testosterone or methyltestosterone. Such assays suggest the androgenicity of oxymetholone is also very low (1/4th to 1/7th its anabolic activity), although real world results in humans suggest it is decidedly higher than that. Oxymetholone is considered by many to be the most powerful steroid commercially available. A steroid novice experimenting with this agent is likely to gain 20 to 30 pounds of massive bulk, and it can often be accomplished within 6 weeks of use. This steroid produces a lot of water retention, so a good portion of this gain is going to be water weight. This is often of little consequence to the user, who may be feeling very big and strong while taking oxymetholone. Although the smooth look that results from water retention is often not attractive, it can aid quite a bit to the level of size and strength gained. The muscle is fuller, will contract better, and is provided a level of protection in the form of extra water held into and around connective tissues. This will allow for more elasticity, and will hopefully decrease the chance for injury when lifting heavy. It should be noted, however, that a very rapid gain in mass might also place too much stress on your connective tissues. The tearing of pectoral and biceps tissue is commonly associated with heavy lifting while massing up on steroids, and oxymetholone is a common offender. There can be such a thing as gaining too fast.
| Brand name | Oxymetholone, Anapolon, Oxymetholone-Alhavi, Oxymetholone IH, Oxyanabolic, Androlic, Anapolon, Oxybolone, Oxitoland, Hemogenin, Synasteron | |||
| Androgenic | 45 | |||
| Anabolic | 320 | |||
| Standard | Methyltestosterone (oral) | |||
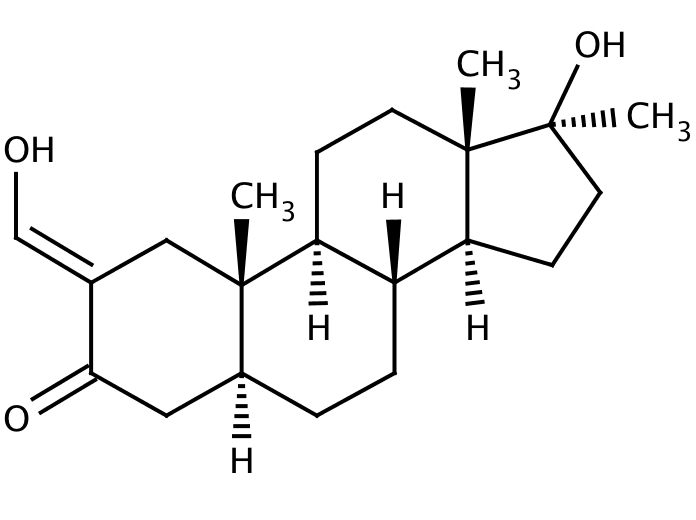
| Chemical Names | 2-hydroxymethylene-17a-methyl-dihydrotestosterone 4,5-dihydro-2hydroxymethylene-17-alpha-methyltestosterone 17alpha-methyl-2-hydroxymethylene-17-hydroxy-5alpha-androstan-3-one | |||
| Estrogenic Activity | high | |||
| Progestational Activity | not significant |
Oxymetholone History
Oxymetholone was first described in 1959.The agent was released in the United States as a prescription drug during the early 1960’s, sold under the brand names Anadrol-50 (Syntex) and Androyd (Parke Davis & Co.). Syntex developed the agent, and would hold patent rights to it until their expiration many years later. The drug was originally approved for use in conditions where anabolic action was necessary. Indicated uses included geriatric debilitation, chronic underweight states, pre- and postoperative preservation of lean mass, convalescence from infection, gastrointestinal disease, osteoporosis, and general catabolic conditions. The recommended dose for such uses was usually 2.5 mg three times per day. The drug was originally supplied in a 2.5 mg, 5 mg, or 10 mg tablet.
In spite of the many potential therapeutic uses or a strong anabolic activity of this drug, the FDA soon strictly narrowed the indicated uses of oxymetholone. By the mid-1970’s, the drug was FDA approved only for the indicated treatment of anemia characterized by deficient red blood cell (RBC) production. Admittedly the stimulation of erythropoiesis is an affect that is characteristic of nearly all anabolic steroids, which as a group tend to increase affect that is characteristic of nearly all anabolic steroids, which as a group tend to increase RBC concentrations. Oxymetholone, however, seemed fairly reliable in this regard; demonstrating an increase in erythropoietin levels as much as 5 fold. This has led to its adoption for this relatively new medical use, as well as the institution of a higher (50 mg) dosage with the updated Anadrol-50 product, necessary for a stronger effect on RBC count. The Parke Davis item would not be brought up to the higher dosage, however, and was discontinued.
Recent years have brought fourth a number of new treatments for anemia, most notably Epogen (recombinant erythropoietin) and related erythropoietic peptides. These drugs directly mimic the body’s natural red blood cell producing hormone, and as such provide a much more focused form of therapy, with less of the unrelated side effects one would have to endure with the use of a strong androgen. Although Anadrol was once viewed as an effective drug for this purpose, sales were now dropping. Financial disinterest finally prompted Syntex to halt production of the U.S. Anadrol 50 in 1993, which was around the same time they decided to drop this item in a number of foreign countries. Plenastril from Switzerland and Austria were dropped; following soon was Oxitosona from Spain. During the mid-1990’s, many Athletes feared oxymetholone was on the way out for good.
In July 1997, Syntex sold all rights to Anadrol-50 in the U.S., Canada, and Mexico to Unimed Pharmaceuticals. Unimed reintroduced Anadrol-50 to the U.S. market in 1998, this time targeting HIV/AIDS patients. Patients with HIV are commonly anemic, often caused by the disease itself, opportunistic infections, or the antiretroviral drugs used to treat the disease. The anemia in HIV patients is typically categorized by impaired red blood cell production in bone marrow, the FDA approved indication for oxymetholone use. Adding to this, oxymetholone was showing great promise in studies combating HIV associated wasting. Unimed soon initiated Phase II/III trials with Anadrol for HIV wasting syndrome, and continued to research its use for treating such things as chronic obstructive pulmonary disease and lipodystrophy (a disorder characterized by a selective loss of body fat, insulin resistance, diabetes, high triglycerides levels, and a fatty liver).
In April 2006, Solvay Pharmaceuticals (parent company of Unimed) sold the rights to Anadrol-50 to Alaven Pharmaceutical, LLC. Alaven continues to market the drug in the United States, although given the transition it is uncertain what additional uses the company plans to pursue with oxymetholone. At the present time the only FDA approved indication remains that of treating red blood cell deficient anemia. Syntex seems to have removed itself from the oxymetholone market globally, discontinuing product or transferring license to other companies whenever possible. Oxymetholone remains available outside of the United States, although it is mostly still sold in smaller and less tightly regulated markets.
How is Oxymetholone Supplied
Oxymetholone is available in select human drug markets. Composition and dosage may vary by country and manufacturer. Most brands contain 50 mg of steroid per tablet.
Structural Characteristics of Oxymetholone
Oxymetholone is a modified form of dihydrotestosterone. It differs by 1) the addition of a methyl group at carbon 17-alpha, which helps protect the hormone during oral administration, and 2) the introduction of a 2-hydroxymethylene group, which inhibits its metabolism by the 3-hsd enzyme and greatly enhances the anabolic and relative biological activity of methyldihydrotestosterone.
Oxymetholone Side Effects (Estrogenic)
Oxymetholone is a highly estrogenic steroid. Gynecomastia is often a concern during treatment, and may present itself quite early into a cycle (particularly when higher doses are used). At the same time water retention can become a problem, causing a notable loss of muscle definition as both subcutaneous water retention and fat levels build. To avoid strong estrogenic side effects, it may be necessary to use an anti-estrogen such as Nolvadex and Arimidex will, likewise, not effect the relative estrogenicity of this steroid. Some have suggested that the high level of estrogenic activity in estrogenicity of this steroid. Some have suggested that the high level of estrogenic activity in oxymetholone is actually due to the drug acting as a progestin, similar to nandrolone. The side effects of both estrogens and progestins can be very similar, which might have made this explanation a plausible one. There was a medical study examining the progestational activity of oxymetholone, however, and it determined that there was no such activity present. With such findings, it seems most plausible that oxymetholone can activate the estrogen receptor, similar to, but more profoundly than, the estrogenic androgen methandriol.
Oxymetholone Side Effects (Androgenic)
Although oxymetholone is classified as an anabolic steroid, androgenic side effects are still possible with this substance. These may include bouts of oily skin, acne, and body/facial hair growth. Higher doses are more likely to cause such side effects. Anabolic/androgenic steroids may also aggravate male pattern hair loss. Women are additionally warned of the potential virilizing effects of anabolic/androgenic steroids. These may include a deepening of the voice, menstrual irregularities, changes in skin texture, facial hair growth, and clitoral enlargement. While Anadrol is classified as an anabolic steroid, it does retain a notable androgenic component.
It is interesting to note that oxymetholone does exhibit some tendency to convert to dihydrotestosterone in the body, although this does not occur via the 5-alpha reductase enzyme. Oxymetholone is already a dihydrotestosterone-based steroid, so no such alteration can take place. Aside from the added c-17 alpha alkylation (discussed below), oxymetholone differs from DHT only by the addition of a 2-hydroxymethylene group. This grouping can be removed metabolically, reducing oxymetholone to the potent androgen 17alpha-methyl dihydrotestosterone (mestanolone). There is little doubt that this biotransformation contributes at least on some level to the androgenic nature of this steroid. Note that since 5-alpha reductase is not involved, the relative androgenicity of oxymetholone is not affected by the concurrent use of finasteride.
Oxymetholone Side Effects (Hepatotoxicity)
Oxymetholone is a c17-alpha alkylated compound. This alteration protects the drug from deactivation by the liver, allowing a very high percentage of the drug entry into the bloodstream following oral administration. C17-alpha alkylated anabolic/androgenic steroids can be hepatotoxic. Prolonged or high exposure may result in liver damage. In rare instances life-threatening dysfunction may develop. It is advisable to visit a physician periodically during each cycle to monitor liver function and overall health. Intake of c17-alpha alkylated steroids is commonly limited to 6-8 weeks, in an effort to avoid escalating liver strain.
Oxymetholone has a saturated A-ring, which slightly reduces its relative hepatotoxicity.388 Still, this agent, particularly at the doses commonly used, can present substantial hepatotoxicity to the user. Studies administering 50 mg or 100 mg daily to 31 elderly men for 12 weeks produced significant increases in liver enzymes (transaminases AST and ALT) only in patients taking 100 mg. A second study administering 50 mg daily to 30 patients for up to and exceeding one year (in some patients) has demonstrated elevations in yglutamyltransferase (GGT) in 17% of patients, significant increases in bilirubin in 10%, andserum albumin increases in 20%.389 One patient developed a liver tumor that could have been peliosis hepatitis, a life-threatening adverse event characterized by blood filled cysts in the liver. A small number of other cases of peliosis hepatitis have been linked to oxymetholone, suggesting the potential for hepatotoxicity should still be carefully considered before use.
The use of a liver detoxification supplement such as Liver Stabil, Liv-52, or Essentiale Forte is advised while taking any hepatotoxic anabolic/androgenic steroids.
Oxymetholone Side Effects (Cardiovascular)
Anabolic/androgenic steroids can have deleterious effects on serum cholesterol. This includes a tendency to reduce HDL (good) cholesterol values and increase LDL (bad) cholesterol values, which may shift the HDL to LDL balance in a direction that favors greater risk of arteriosclerosis. The relative impact of an anabolic/androgenic steroid on serum lipids is dependant on the dose, route of administration (oral vs. injectable), type of steroid (aromatizable or non-aromatizable), and level of resistance to hepatic metabolism. Anabolic/androgenic steroids may also adversely affect blood pressure and triglycerides, reduce endothelial relaxation, and support left ventricular hypertrophy, all potentially increasing the risk of cardiovascular disease and myocardial infarction.
Oxymetholone has a strong effect on the hepatic management of cholesterol due to its structural resistance to liver breakdown and route of administration. Studies administering 50 mg or 100 mg daily to a group of elderly men for 12 weeks have demonstrated insignificant increases in LDL cholesterol, accompanied by very significant (dramatic) suppressions of HDL cholesterol (reduced 19 and 23 points in the 50 mg and 100 mg groups, respectively). The use of oxymetholone should be undertaken only after careful consideration in people with high cholesterol or a familial history of heart disease.
To help reduce cardiovascular strain it is advised to maintain an active cardiovascular exercise program and minimize the intake of saturated fats, cholesterol, and simple carbohydrates at all times during active AAS administration. Supplementing with fish oils (4 grams per day) and a natural cholesterol/antioxidant formula such as Lipid Stabil or a product with comparable ingredients is also recommended.
Oxymetholone Side Effects (Testosterone Suppression)
All anabolic/androgenic steroids when taken in doses sufficient to promote muscle gain are expected to suppress endogenous testosterone production. Without the intervention of testosterone stimulating substances, testosterone levels should return to normal within 1-4 months of drug secession. Note that prolonged hypogonadotrophic hypogonadism can develop secondary to steroid abuse, necessitating medical intervention.
Note that when discontinuing oxymetholone, the crash can be as equally powerful as the oncycle results. To begin with, the level of water retention will quickly diminish, dropping the user’s body weight dramatically. This should be expected, and not of much concern. What is usually of most concern is restoring endogenous testosterone production with a proper PCT program (see: Post Cycle Therapy in this book). Before going off, some alternately choose to first switch over to a milder injectable like Deca-Durabolin for several weeks. This is in an effort to “harden up the new mass,”and can prove to be an effective practice, at least from a mental standpoint. A drop of weight is likely when making the switch, although the end result is still often viewed as allowing the retention of more (quality) muscle mass. It is sort of stepping down, first off the water retention, and weeks later finally off the hormones. Remember ancillaries though, as testosterone production will not be rebounding during Deca therapy.
Oxymetholone Administration (General)
Studies have shown that taking an oral anabolic steroid with food may decrease its bioavailability. This is caused by the fat-soluble nature of steroid hormones, which can allow some of the drug to dissolve with undigested dietary fat, reducing its absorption from the gastrointestinal tract. For maximum utilization, this steroid should be taken on an empty stomach.
Oxymetholone Administration (Men)
Early prescribing guidelines for oxymetholone recommended a dosage of 2.5 mg three times per day to reverse the wasting process and provide lean body mass gain. Doses as high as 30 mg were employed in some cases. Current prescribing guidelines recommend a dosage of 1-5 mg per kilogram of bodyweight per day for treating anemia, although indicate that a dose of 1-2 mg/kg is typically sufficient. A 175-pound person would take approximately 150 mg per day at the 2 mg/kg dosage level. In some other countries, it is recommended to limit the dosing of oxymetholone to 100 mg per day. Therapy is usually given for a minimum of three to six months.
When used for physique- or performance-enhancing purposes, an effective oral daily dosage would fall in the range of 25-150 mg, taken in cycles lasting no more than 6-8 weeks to minimize hepatotoxicity. This level is sufficient for dramatic increases in muscle mass and strength. Higher doses are rarely administered due to the strong estrogenic nature of the drug, as well as the high potential for hepatotoxicity. When used for physique- or performance-enhancing purposes, an effective oral daily dosage would fall in the range of 25-150 mg, taken in cycles lasting no more than 6-8 weeks to minimize hepatotoxicity. This 25-150 mg, taken in cycles lasting no more than 6-8 weeks to minimize hepatotoxicity. This level is sufficient for dramatic increases in muscle mass and strength. Higher doses are rarely administered due to the strong estrogenic nature of the drug, as well as the high potential for hepatotoxicity.
Oxymetholone Administration (Women)
Prescribing information for oxymetholone in the U.S. makes no distinction with the dose for females. Oxymetholone is generally not recommended for women for physique- or performance enhancing purposes due to its very strong nature and tendency to produce virilizing side effects.
Oxymetholone Availability
Pharmaceutical preparations containing oxymetholone are fairly limited. The legitimate supply seems to be scattered into isolated markets of Europe, Asia, and the Americas. Most of the supply for this drug comes in the form of underground and export-only products. In reviewing some of the remaining products and changes in the legitimate global pharmaceutical market, we have made the following observations.
Anapolon (Turkey) was recently updated to reflect a new logo for the manufacturer Abdi Ibrahim. The product is still packaged in boxes of 20 tablets each.
Anadroxyl from Kalpa Pharmaceuticals. It contains 50 mg of steroid per tablet, with 50 packaged in a sachet. This product is widely distributed online.
Oxymetholone-Alhavi (Iran) was recently updated. It is now packaged in foil and plastic strips of 10 tablets each, 10 strips per box.
Oxymetholone IH (Iran Hormone) was also updated recently. The presentation remains similar (strips of 10 tablets, 10 per box), though the box looks more modern with gradient coloring.
Oxydrol from British Dragon. It contains 50 mg of steroid per tablet, with 50 packaged in a sachet. This product is widely distributed online.
Oxyanabolic from Asia Pharma (Malaysia) is now registered for sale in Thailand.The product comes in strips of 10 tablets, each with an embedded AP and 50. The product should also carry a unique product ID number that can be verified on the company website.
Oxyplex from Axiolabs. It contains 50 mg of steroid per tablet, with 50 packaged in a sachet. This product is widely distributed online.
Androlic from British Dispensay (Thailand) is also still in production. The product comes in bottles of 100 tablets each. The tablets are green, scored on one side, and stamped with the BD snake emblem logo on the other. The product carries a holographic sticker to deter counterfeiting, though even this sticker has been duplicated with high accuracy.
Balkan Pharmaceuticals (Moldova) makes the product Anapolon. It is prepared in 50 mg tablets, with 20 tablets contained in each foil and plastic strip.
Oxydex from Sciroxx. It contains 50 mg of steroid per tablet, with 50 packaged in a sachet. This product is widely distributed online.
Oxybolone from Genepharm Greece is again in production. It contains 50 mg of steroid per tablet, with 10 packaged in each foil and plastic blister. Two strips are packed in each box. This product is widely distributed through export.
Oxitoland is manufactured in Paraguay by Laboratorio Farmaceutico/Landerlan. Each box holds 2 strips foil and plastic blisters of 10 tablets each.
Oxymetholone is produced by Swiss Remedies and available across Europe. Due to numerous fakes of this product, Swiss Remedies offers a convenient online product checker.
Magnus Pharmaceuticals makes the product Oxymetholone primarily for the EU and UK markets. Due to fake products appearing on the market, Magnus offers an online checker that lets steroid users verify their product originality.
Bodybuilders reference
This is an oral 17-alfa-alkylated steroid that is highly androgenic and highly anabolic. Reported gains in body weight of up to 20 LBS in the first 3 weeks of use were not uncommon. Athletes using this drug experienced remarkable strength and recovery elevations. Users noted a distinct increase in aggressiveness, (which if focused on training only was noted as positive) excessive water retention, and muscular size. Oxymetholone is commonly used as an off season mass building drug, though some mass monsters have used it up to 7-10 days before competition by stacking antagonist anti- estrogens and diuretics.
Unfortunately this drug is probably the most dangerous of all AAS when abused and utilized when not under a physician’s care. Users get huge but often feel flu-like symptoms during use. Oxymetholone abuse is linked to prostate and liver cancer, liver disease, thyroid dysfunction, leukemia, and heart disorders. Even hepatic coma can result from abuse. Not uncommon side effects included: sensitivity to anti-coagulants (the stuff that regulates bleeding internally and externally) hair loss, prostate enlargement, severe suppressions of the HPTA resulting in low sperm and endogenous (natural) androgen production, nausea, stomach aches, diarrhea, and throwing up on occasion. Women can add possible virilizing symptoms such as clitoral enlargement, facial hair growth, deeper voice, missed periods, and other androgenic linked side-effects.
Oxymetholone negatively effects liver function such as an increase in SGPT and SGOT enzymes which are indications of hepatitis (liver infections) which can manifest itself as yellowing of the eyes and finger nails because of an increase in biliburin in the liver. Another liver enzyme, gamma -GT, is sensitive to Oxymetholone, and alkaline phosphatase is altered as well. I cannot stress the importance of monitoring by a doctor.
Oxymetholone is a derivative of DHT. Many report gyno from use but this is unlikely due to this drug aromatizing because DHT does not aromatize to estrogen. The more likely reason is they purchased bogus oxymetholone from a black market dealer that actually contained methyltestosterone. There is another reason gyno is possible, but we will discuss that in a moment. Oxymetholone does cause high water retention due to electrolyte retention thus creating a massive but puffy appearance to muscles. For the same reason, the drug causes water retention and fluid build up in joints. This manifests itself in joint pain-free training for most users. In medicine Oxymetholone is used to treat low red blood cell production which means during administration red blood cell count is stimulated. For this reason the drug increases oxygen transport to the muscles resulting in an incredible muscle pump after only a few sets of training. I have often noted those who used oxymetholone recovered between sets, exercises, and work-outs at a remarkable rate. So the drug does protect against overtraining quite well, thus when it was stacked with anti-estrogen such as Nolvadex and a diuretic to cut electrolyte (aldosterone) caused water retention, and a high anabolic drug such as Deca Durabolin, quality, quantitative, muscle gain resulted. The fact that this drug’s water retention side effect responds to antagonist type anti-estrogens is interesting since, from a chemical structure stand-point, it should not aromatize to estrogen. Even the insert states edemas (water retention) may occur but does not list elevated estrogen levels under “side effects”. However, readers should realize Oxymetholone itself can merge with Progesterone receptors and may act as an estrogen in this manner.
As to dosages, advanced bodybuilders and power lifers usually reported excellent results with 50-200 mg daily divided in 2-3 dosages. Since results begin to decline after the first 2 weeks it some reported that their protocols were more productive (and safer) when they started at 50mg daily and increase by one tab weekly until a total of 150-200 mg daily was reached at week 3. They then maintained that dosage for a total of 2-3 additional weeks. Some reported a following protocol that allowed reduced dosages by one tab weekly. My personal experience has been that liver stress becomes an issue after the 4th week of administration and as such did not personally exceed this time period for use. Replacing Oxymetholone with a high anabolic such as Deca Durabolin or Equipoise during the transitional phase was quite effective for maintaining a greater amount of the oxymetholone induced lean mass. Many reported exceptional results with a stack consisting of 50-100 mg oxymetholone daily, 152-228 mg of Parabolon weekly, and 200- 500 mg of testosterone enethate weekly.
Women should not use oxymetholone, but of course some hard core types did report self administration. Novice steroid users should never use oxymetholone without a doctors supervision.
In most cases users reported that liver values returned to normal after 1-2 months of discontinued. This seems to be supported by the available medical literature on oxymetholone. High blood pressure was common during use. High blood pressure should never go untreated. The hair loss does not reverse by the way. Post-cycle the administration of HCG and Clomid was used to return normal HPTA function in all but very rare cases. “The boys” normally began to produce normal sperm and testosterone levels after 2-3 weeks of discontinuance. Can you tell that I did not like Oxymetholone for long term personal use? Post-cycle, without the layering of a transitional phase replacement AAS such as nandrolones, Primobolan Depot, Equipoise or Winstrol Depot, gains made with Oxymetholone alone soon disappear in most cases. (See “Max Androgen Phases” in “Building The Perfect Beast” for a discussion of solutions some hard-core types have utilized).
A note of interest: There is not a “legit” injectable form of Oxymetholone. However, it would be very physiologically active as is the 25mg sublingual form. I have used a MEGA- MIX product that contained Oxymetholone in a 3 oil mix injectable that was a black- market product with excellent results and fewer negative side effects. However, black market manufactured AAS are often dangerous and unlikely legal anywhere.
Anabolic Steroid Guide reference
Anadrol 50 is the strongest and, at the same time, also the most effective oral steroid. The compound has an extremely high androgenic effect which goes hand in hand with an extremely intense anabolic component. For this reason, dramatic gains in strength and muscle mass can be achieved in a very short time. An increase in body weight of 10 – 15 pounds or more in only 14 days is not unusual. Water retention is considerable, so that the muscle diameter quickly increases and the user gets a massive appearance within record time. Since the muscle cell draws a lot of water, the entire muscle system of most athletes looks smooth, in part even puffy. Anadrol does not cause a qualitative muscle gain but rather a quantitative one which in the off-season is quite welcome. Anadrol “lubricates” the joints since water is stored there as well. On the one hand this is a factor in the enormous increase of strength and, on the other hand, it allows athletes with joint problems a painless workout. Powerlifters in the higher weight classes are sold on Anadrol. A strict diet, together with the simultaneous intake of Nolvadex and Proviron, can significantly reduce water retention so that a distinct increase in the solid muscles is possible. By taking Anadrol the athlete experiences an enormous “pump effect” during the workout in the exercised muscles. The blood volume in the body is significantly elevated causing a higher blood supply to the muscles during workout. Anadrol increases the number of red blood cells, allowing the muscle to absorb more oxygen. The muscle thus has a higher endurance and performance level. Consequently, the athlete can rely on great power and high strength even after several sets. The highly androgenic effect of Anadrol stimulates the regeneration of the body so that the often-feared “overtraining” is unlikely. Although Anadrol is not a steroid used in preparation for a competition, it does help more than any other steroid during dieting to maintain the muscle mass and to allow an intense workout. Many bodybuilders therefore use it up to about one week before a competition, solving the problem of water retention by taking antiestrogens and diuretics so that they will appear bulky and hard when in the limelight.
As for the dosage, opinions differ. A dosage sufficient for any athlete would be 0,5 – 0,8 mg per pound of body weight/day. This corresponds to 1-4 tablets; i.e. 50-200 mg/day. Under no circumstances should an athlete take more than four tablets in any given day. We are of the opinion that a daily intake of three tablets should not be exceeded. Those of you who would like to try Anadrol 50 for the first time should begin with an intake of only one 50 mg tablet. After a few days or even better, after one week, the daily dosage can be increased to two tablets, one tablet each in the morning and evening, taken with meals. Athletes who are more advanced or weigh more than 220 pounds can increase the dosage to 150 mg/day in the third week. This dos-age, however, should not be taken for periods longer than two to three weeks. Anadrol 50 should not exceed six weeks. After discontinuing Anadrol, it is important to continue steroid treatment with another compound since, otherwise, a drastic reduction takes place and the user, as is often observed, within a short period looks the same as before the treatment. No other anabolic/androgenic steroid causes such a fast and drastic loss in strength and mass as does Anadrol 50. Athletes continue their treatment with injectable testosterone such as Sustanon 250 or Testosterone enanthate for several weeks. Bodybuilders often combine Anadrol with Deca- Durabolin or Testosterone to build up strength and mass. A very effective stack which is also favored by professionals consists of Anadrol 100 mg +/day, Parabolan 228 mg +/week, and 5ustanon 500 mg +/week. This stack quickly improves strength and mass but it is not suitable for and steroid novices. Anadrol 50 is to be taken seriously and the prevailing bodybuilder mentality “more is better” is out of place.
Anadrol 50 is unfortunately also the most harmful oral steroid. Its intake can cause many considerable side effects. Since it is I 7-alpha alkylated it is very liver-toxic. Most users can expect certain pathological changes in their liver values after approximately one week. An increase in liver values of both the enzymes GOT and GPT also called transaminases, often cannot be avoided. Elevated GOT and GPT values are indications of hepatitis, i.e. a liver infection. Those who discontinue oxymetholone will usually show normal values within two months. Longer intake and/or higher doses can cause a yellow discoloration of fingernails, eyes, or skin jaundice). This is because oxymetholone induces an increase of biliburin in the liver, producing a bile pigment which causes the yellow discoloring of the skin. The liver enzyme gamma-GT also reacts sensitively to the oxymetholone, causing it to elevate. If high dosages of Anadrol 50 are taken over a long period, there is an increased risk that the described liver changes could end up damaging the liver. During the intake of Anadrol 50, the liver values, GOT, GPT, bilirubin, gamma-GT and alkaline phosphatase (AP), as well as the LDH/HBDH quotient, should always be checked by a competent physician. Anadrol 50 (representing all oxymetholone-containing steroid products) is the only anabolic/androgenic steroid which was linked with liver cancer.
The compound oxymetholone easily converts into estrogen. This causes signs of feminization (e.g. gynecomastia) and the already mentioned water retention which in turn requires the intake of antiestrogens (e.g. Nolvadex and Proviron) and an increased use of diuretics (e.g. Lasix) before a competition. The increased water retention, in addition to the aesthetical problems, can be further detrimental since it may cause high blood pressure. In extreme cases the intake of an anti-hypertensive drug, e.g. Catapresan, may be necessary. Oxymetholone doesn’t convert to DHT. However, it is a potent androgen. Bodybuilders who experience severe steroid acne caused by Anadrol can get this problem under control by using the prescription drug Accutane. Other possible side effects may include headaches, nausea, vomiting, stomach aches, lack of appetite, insomnia, and diarrhea. The athlete can expect a feeling of “general indisposition” with the in-take of Anadrol which is completely in contrast to Dianabol which conveys a “sense of well-being”. The increased aggressiveness is caused by the resulting high level of androgen and occurs mostly when large quantities of testosterone are “shot” simultaneously with the Anadrol. The body’s own production of testosterone is considerably reduced since Anadrol has an inhibiting effect on the hypothalamus, which in turn completely reduces or stops the release of GnRH (gonadotropin releasing hormone). For this reason the intake of testosterone-stimulating compounds such as HCG and Clomid is absolutely necessary to main-tain the hormone production in the testes.
Anadrol 50 is not recommended for women since it causes many and, in part, irreversible virilizing symptoms such as acne, clitorial hypertrophy, deep voice, increased hair growth on the legs, beard growth, missed periods, increased libido, and hair loss. Anadrol is simply too strong for the female organism and accordingly, it is poorly tolerated.
Newbies Research Guide reference
Anadrol was the U.S. brand name for 50mg Oxymetholone tablets, which were available in the U.S. until 1993. Syntex is the world producer of this drug, and markets it under a few different brand names in other areas. Oxymetholone is a 17alpha alkylated oral steroid. Second to none, this product is generally con- sidered the most powerful steroid available. Anadrol will produce extremely dramatic weight and strength gains in its user. Some of this weight and strength gain will be due to the drugs heavy water retention. Users of Anadrol report severe crashes when stopping usage, mostly due to the loss of water and inhibited endogenous hormone production brought about during the cycle. Aside from the water, Anadrol will pack on the mass like no other steroid. A short cycle of Anadrol could account for a gain of over 20lbs in many users, sometimes more. As this drugs anabolic properties are so extreme, so are it’s androgenic side effects. Due to the strength of these side effects, Anadrol should never be used by women. For starters, oxymetholone will easily convert to estrogen and DHT. As stated earlier water retention will be present, along with an increase in blood pressure. Kidney functions may also need to be looked after during longer use. Hair loss has also been reported among users with a predisposition for male-pattern baldness. The most dangerous attribute of Anadrol is that is it 17alpha alkylated. As you probably know 17aa orals are toxic to the liver. Unlike Dianabol (another popular 17aa oral) which is effective in doses of as little as 15mg, Anadrol users generally start with 50mg/day and often lead up to 150mg/day. So when a user takes 3 Anadrol tablets, his liver is processing roughly the equivalent of 30 Dianabol tablets. This obviously is quite a lot of 17aa steroid for your liver to process, so it is pertinent a user has his liver enzymes checked regularly with a doctor. When you hear of horror stories involving liver cancer from steroid use, Anadrol is most often the culprit. For medical treatment, Syntex recommends 1-5mg/kg of bodyweight per day. This leads many patients to take as many as 8+ tabs per day, for extended periods of time. This is much more than an athlete would need and should be using, which may be why documented cases of liver cancer seem more prominent among non-athletes taking Anadrol medically. Lately, many people are speculating on how long this product will be available worldwide. Syntex has stopped production of Anadrol in the U.S., Oxitosona in Spain and medical use in other areas of the world seems to be declining due to the advent of newer drugs to treat conditions in which Anadrol was formerly used.
Aside from the Mexican version, all other forms of Anadrol are now being counterfeited, often with incredible accuracy. In the U.S., a version of the now unavailable American Anadrol has been found in which box, bottle and even the stamping of the tablet are identical to the real version. The only seen differ- ence is the lack of active ingredient. Since real U.S. Anadrol has been out of production for some time, it would be safe to say anything labeled Anadrol is fake. Anapolon is copied as well with good accuracy. Oxitosona was/is counterfeited but since Syntex dropped its production in 1993, all forms should be considered fake. Hemogenin from Brazil is another popular version, which makes its way to the states and is also counterfeited. Currently, all the loose red Anadrols from Mexico (Stamped with SYNTEX on one side and 2902 on the other) which are circulating the states should be considered real. They are avail- able only to clinics and hospitals in Mexico, so black market supplies are limited. Reports are that they may also be slightly underdosed.
This is an oral drug with a dosage of 50mg per tablet. This is the strongest oral on the market. It has both high androgenic and anabolic effects. Strength and weight gains are very significant. Anadrol is highly toxic to the liver. It also aromatizes fairly easily. This drug has been reported to produce gynecomastia in users (not all probably around 50%). An anti-estrogen should be used with this drug to counteract the aromatization. Nolvadex is an anti-estrogen with little to no side effects and it’s talked about later. Many side effects are associated with Anadrol including acne, hair loss, abdominal pains, headaches, gynecomastia, hypertension, and heavy water retention. Loss of weight and strength usually occurs after the cycle. Anadrol also shuts down natural testosterone production. Anadrol is regarded by the bodybuilding community as the most effective oral steroid in building strength and size. Anadrol has many side effects however, which make it relatively dangerous to use when compared to other steroids. If you wish to buy Oxymetholone online by Dragon Pharma, then click here.
References
Wlliam Llewellyn (2011) – Anabolics
L. Rea (2002) – Chemical Muscle Enhancement Bodybuilders Desk Reference
Anabolic Steroid Guide
Newbies Research Guide
Your experience with Anadrol — oxymetholone


About Author
baxx
Doctor Baxx is an internationally recognized leader in the competitive bodybuilding industry. Its advanced bodybuilder and fitness training specialist certification provides beginners with opportunities for further advancing their knowledge and skills with bodybuilding at the advanced level.