Andractim — dihydrotestosterone
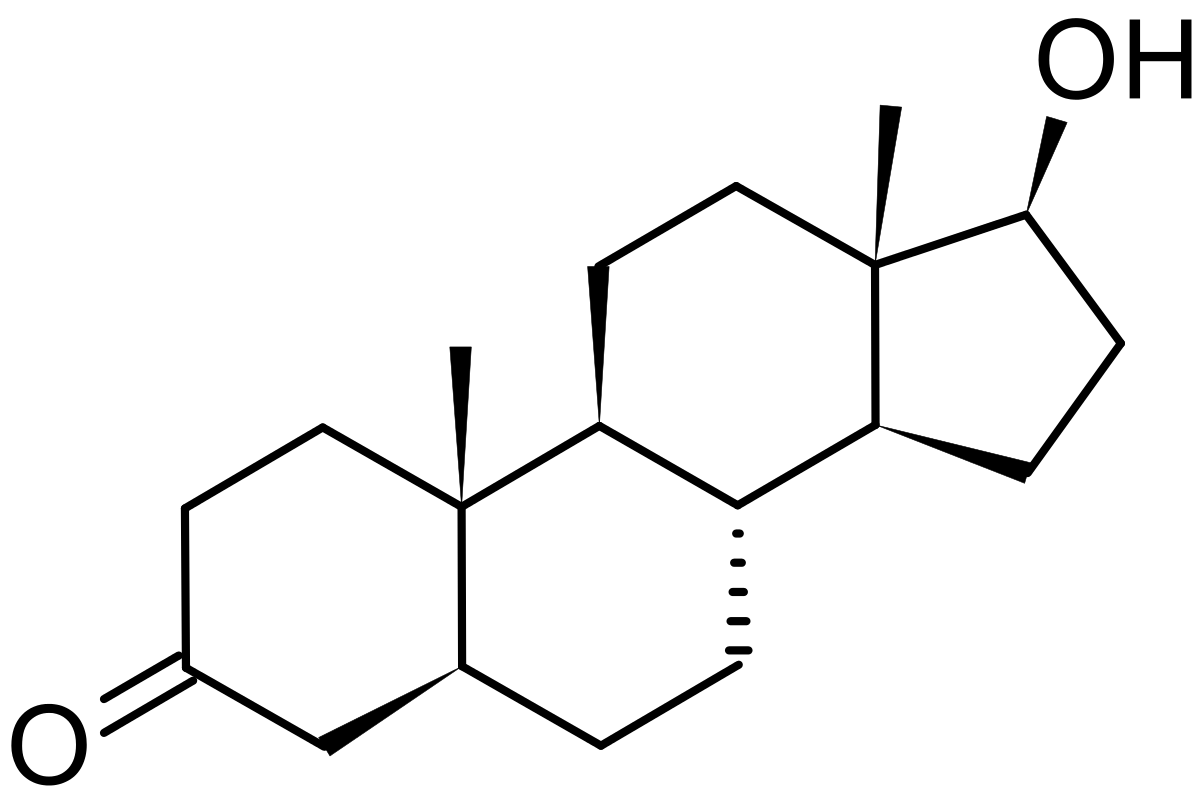
Andractim is a prescription steroid preparation that contains the potent androgenic steroid dihydrotestosterone. This product comes in the form of a transdermal gel, typically containing 2.5% dihydrotestosterone by weight in an 80gram tube. As with Androgel, roughly 10% of the active steroid will make it into circulation with each application.This would equate to 80 doses of 25 mg, with each dose delivering approximately 2.5 mg of steroid to the body. Dihydrotestosterone itself is the most active androgen in the human body, displaying an ability to bind and activate the androgen receptor at least three or four times greater than that of its parent steroid testosterone. This trait, however, is not accompanied by equally powerful anabolic tendencies. In the case of dihydrotestosterone, we have a steroid that is almost purely androgenic, with only minimal muscle-building (anabolic) action. Dihydrotestosterone is a weak muscle builder because it is extremely open to alteration by the 3-alpha-hydroxysteroid-dehydrogenase enzyme, responsible for breaking down active steroids like DHT into their inactive metabolites. 3a-HSD is present in high quantities in muscle tissue, running interference between the outer cell membrane and the androgen receptors that all steroid hormones are trying to reach. In humans, little DHT ends up actually reaching this receptor. Testosterone is very resistant to this enzyme, however, which allows it to be a much more effective muscle-building agent. 3a-HSD steroid deactivation in muscle tissue causes the same problem with Proviron (1-methyl-dihydrotestosterone). DHT and Proviron both have very effective uses in areas such as fat loss, hardening, increasing CNS activity, and pure strength gains, but they do not perform well as anabolic agents.
| Brand name | Dihydrotestosterone, Apeton, Apeton depot | |||
| Androgenic | 30-260 | |||
| Anabolic | 60-220 | |||
| Standard | Testosterone, T. propionate | |||
| Chemical Names | 5-alpha-androstan-3-one-17beta-ol 5-alpha-androstanolone |
|||
| Estrogenic Activity | none | |||
| Progestational Activity | none |
Dihydrotestosterone History
Dihydrotestosterone was first synthesized in 1935. This strong androgen was put into consistent medical use during the late 1950’s, after a series of experiments demonstrating that it had measurable anabolic effects. Prior to this it was largely believed that DHT was exclusively an androgenic substance, and was of little value clinically. Dihydrotestosterone gels were developed more recently, and have been investigated for a number of medical purposes. At present, these preparations are primarily indicated for the treatment of androgen deficiency, gynecomastia, and insufficient genital growth. Transdermal DHT has been successful as an androgen replacement medication in older men at risk for developing prostate hypertrophy largely because of its non-aromatizable nature, as this disorder is fueled partly by estrogens. The latter two indications are considered local applications of the fueled partly by estrogens. The latter two indications are considered local applications of the drug, and the DHT gel is applied directly to the tissues requiring treatment.
The primary manufacturer of dihydrotestosterone gel globally is Besins International, based in France. Besins produces the drug under the Andractim name, selling it in France and scarcely in other parts of Europe. Dihydrotestosterone gels are found much less commonly outside of Europe, and presently no such preparation is commercially available in the United States. In 1995, U.S. manufacturer Unimed Pharmaceuticals purchased the rights to Andractim from Besins in the U.S., Mexico, and Canada. The firm announced an interest in the drug for several uses, including androgen replacement in men over age sixty, treating benign prostate hypertrophy, and combating HIV- associated wasting. Its use as an anabolic may be desirable with HIV because it had been determined that many patients lack an ability to properly convert testosterone to DHT, and therefore lack sufficient levels of this important androgen. It appears that Unimed has since sold its interests in the anabolic steroid market, however, leaving the potential reemergence of dihydrotestosterone in the U.S. in question. How Supplied: Hydroalcoholic transdermal dihydrotestosterone gels are available in select human drug markets. Composition and dosage may vary by country and manufacturer, but usually contain 2.5% dihydrotestosterone by weight. Structural Characteristics: Andractim is a hydroalcoholic gel containing 2.5% of dihydrotestosterone (free) by weight. It is designed to provide a continuous transdermal delivery of dihydrotestosterone for 24 hours following application to the skin. Approximately 10% of the applied dose is absorbed across the skin during each 24-hour period.
How is Dihydrotestosterone Supplied
Hydroalcoholic transdermal dihydrotestosterone gels are available in select human drug markets. Composition and dosage may vary by country and manufacturer, but usually contain 2.5% dihydrotestosterone by weight.
Structural Characteristics of Dihydrotestosterone
Andractim is a hydroalcoholic gel containing 2.5% of dihydrotestosterone (free) by weight. It is designed to provide a continuous transdermal delivery of dihydrotestosterone for 24 hours following application to the skin. Approximately 10% of the applied dose is absorbed across the skin during each 24-hour period.
Dihydrotestosterone Side Effects (Estrogenic)
Dihydrotestosterone is not aromatized by the body, and is not measurably estrogenic. An anti-estrogen is not necessary when using this steroid, as gynecomastia and water retention should not be concerns even among sensitive individuals. DHT also has inherent antiestrogenic properties, competing with other substrates for binding to the aromatase enzyme. Percutaneous dihydrotestosterone may be an effective option for the treatment of gynecomastia. Studies have reported a good level of success when treating certain forms of this disorder with Andractim, the drug affecting the ratio of androgenic to estrogenic action in the breast area enough that a notable regression of mammary tissue has been achieved in many cases.
Dihydrotestosterone Side Effects (Androgenic)
Dihydrotestosterone is the strongest natural male androgen. Higher than normal therapeutic doses are likely to produce androgenic side effects including oily skin, acne, and body/facial hair growth. Men with a genetic predisposition for hair loss (androgenetic alopecia) may notice accelerated male pattern balding. Women are warned of the potential virilizing effects of anabolic/androgenic steroids, especially with a strong androgen such as dihydrotestosterone.These may include deepening of the voice, menstrual irregularities, changes in skin texture, facial hair growth, and clitoral enlargement. Note that the 5-alpha reductase enzyme does not metabolize dihydrotestosterone, so its relative androgenicity is not affected by finasteride or dutasteride.
Dihydrotestosterone Side Effects (Hepatotoxicity)
Dihydrotestosterone does not have hepatotoxic effects; liver toxicity is unlikely.
Dihydrotestosterone Side Effects (Cardiovascular)
Anabolic/androgenic steroids can have deleterious effects on serum cholesterol. This includes a tendency to reduce HDL (good) cholesterol values and increase LDL (bad) cholesterol values, which may shift the HDL to LDL balance in a direction that favors greater risk of arteriosclerosis. The relative impact of an anabolic/androgenic steroid on serum lipids is dependant on the dose, route of administration (oral vs. injectable), type of steroid (aromatizable or non-aromatizable), and level of resistance to hepatic metabolism. Anabolic/androgenic steroids may also adversely affect blood pressure and triglycerides, reduce endothelial relaxation, and support left ventricular hypertrophy, all potentially increasing the risk of cardiovascular disease and myocardial infarction. Therapeutic doses of dihydrotestosterone used to correct insufficient androgen production in otherwise healthy aging men are unlikely to increase atherogenic risk. Higher doses are likely to increase atherogenic risk, but less dramatically than equivalent doses of synthetic oral anabolic/androgenic steroids.
To help reduce cardiovascular strain it is advised to maintain an active cardiovascular exercise program and minimize the intake of saturated fats, cholesterol, and simple carbohydrates at all times during active AAS administration. Supplementing with fish oils (4 grams per day) and a natural cholesterol/antioxidant formula such as Lipid Stabil or a product with comparable ingredients is also recommended.
Dihydrotestosterone Side Effects (Testosterone Suppression)
All anabolic/androgenic steroids when taken in doses sufficient to promote muscle gain are expected to suppress endogenous testosterone production. Without the intervention of testosterone stimulating substances, testosterone levels should return to normal within 1-4 months of drug secession. Note that prolonged hypogonadotrophic hypogonadism can develop secondary to steroid abuse, necessitating medical intervention.
Dihydrotestosterone Administration (Men)
To treat androgen insufficiency, hydroalcoholic transdermal dihydrotestosterone gels have been used in doses ranging from 16 to 64mg per day (1.6-6.4mg of hormone delivered). For physique- or performance-enhancing purposes, higher doses would be necessary to achieve strong supraphysiological levels of dihydrotestosterone. Logical effective doses begin in the range of 50-100 mg per day, or 5-10 mg of hormone delivered systemically. Dihydrotestosterone is of little value for building muscle, and is most commonly applied for cutting or pure-strength-promoting purposes.
Dihydrotestosterone Administration (Women)
Hydroalcoholic transdermal dihydrotestosterone gel is not recommended for women for physique- or performance-enhancing purposes due to its strong androgenic nature and tendency to produce virilizing side effects.
Dihydrotestosterone Availability
Pharmaceutical preparations containing transdermal dihydrotestosterone gel remain scarce. The legitimate supply seems to be scattered into isolated markets of Europe, Asia, and South America. In reviewing some of the remaining products and changes in the global pharmaceutical market, we have made the following observations.
One of the most notable preparations is Andractim from Besins-Iscovesco in France. It contains 25 mg/mL of hormone in a 100 gram tube.
Andractim is produced in Belgium by Piette. It contains 25 mg/mL of hormone in an 80 gram tube.
Andractim is produced in India by Chemec. It contains 25 mg/mL of hormone in a 100 gram tube.
Bodybuilders reference
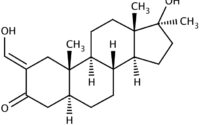
This was a rarely used or available drug. Since it is almost identical to DHT, it cannot convert to estrogen. Water retention is rare for the same reason. As a strength or weight gain drug, androstanolone is of no value unless dosages are increased significantly. In this case the individuals whom have used larger dosages have reported significant increases in strength and muscle quality similar to those realized during utilization of so-called contest prep drugs like trenbolones and Masteron. (Both will be reported upon later in this text)
This has not been a commonly used drug simply due to cost. If the economic issues had been resolved some reported the drug would be a common replacement for socalled hardening AAS. However, some women have replied that they have used it with moderate success as a pre-contest hardening drug in the listed average reported dosages. For this to be successful, a very low body fat level was achieved first.
There is an OTC product available in the United States that is chemically almost identical to the oral androstanolone. It is called Hyroxy-Bolasterone. Interestingly enough, it is my personal opinion from experience that it is a more effective product with fewer potential negative side effects.
Anabolic Steroid Guide reference
Androstanolone is identical to the body’s own dihydrotestosterone which, as we know, is formed by the peripheral conversion of testosterone. Some therefore call Androstanolone a synthetic dihydrotestosterone. This steroid has a predominantly androgenic effect and, due to its structure, cannot be converted into estrogen. For a fast buildup of power and muscle mass Androstanolone is of little value. It used to be the athlete’s favorite competition steroid since it helped to obtain a harder muscle through a lower fat content by increasing the androgen level without aromatizing. Numerous athletes used Androstanolone during workouts for dopingtested championships since the substance remains in the body for only a short time and the testosterone/epitestosterone value is not influenced. Another positive characteristic is that the injectable version is not liver-toxic. Today, however, Androstanolone is rarely used by athletes. One reason for this is that almost all European and American compounds are no longer commercially available. The other reason is that most athletes use the still readily available Masteron which has similar effects. Neither the original nor a fake of Androstanolone is available on the black market.
References
Wlliam Llewellyn (2011) – Anabolics
L. Rea (2002) – Chemical Muscle Enhancement Bodybuilders Desk Reference
Anabolic Steroid Guide
Your experience with Andractim — dihydrotestosterone

About Author
baxx
Doctor Baxx is an internationally recognized leader in the competitive bodybuilding industry. Its advanced bodybuilder and fitness training specialist certification provides beginners with opportunities for further advancing their knowledge and skills with bodybuilding at the advanced level.