Anatrofin — stenbolone acetate
Stenbolone acetate is an injectable anabolic steroid derived from dihydrotestosterone. Stenbolone was actually developed on a 1 -testosterone backbone, differing only by the addition of a 2-methyl group. The resulting steroid remains very similar to its non-methylated base, with only modest differences in anabolic and androgenic potency. On the tissue-building side, stenbolone is probably a little weaker on a milligram for milligram basis than 1-testosterone, although it is difficult to make direct comparisons. As an androgen, stenbolone is also probably slightly weaker than 1-testosterone, when you are talking milligram for milligram dose, although the anabolic/androgenic ratio (the more relevant measure) remains very similar. When compared to testosterone, standard assays suggest that stenbolone has roughly three times greater anabolic effect, and somewhere between 15% and 30% more androgenic activity.
| Brand name | Anatrofin, Stenbolone acetate | |||
| Androgenic | 115-130 | |||
| Anabolic | 300 | |||
| Standard | Testosterone | |||
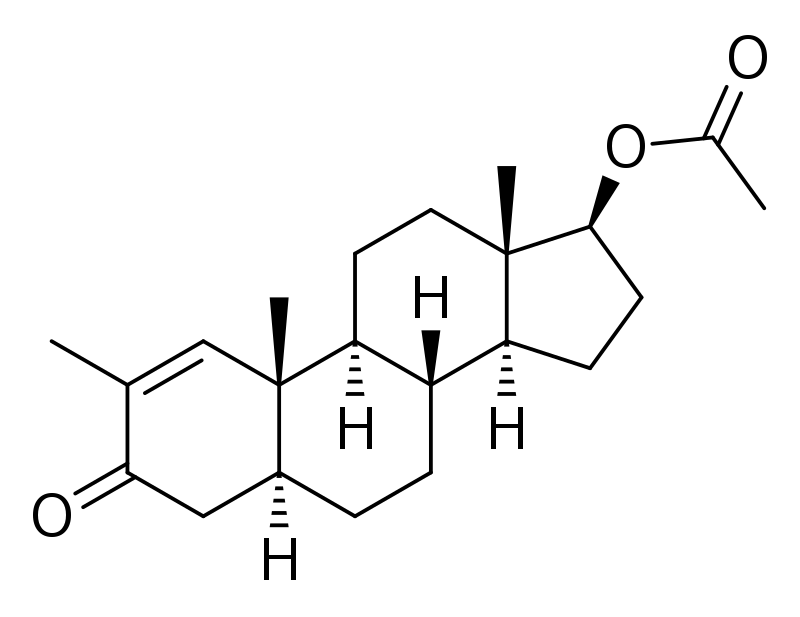
| Chemical Names | 2-methyl-5a-androst-1-en-17b-ol-3-one | |||
| Estrogenic Activity | none | |||
| Progestational Activity | no data available |
Anatrofin History
Schering AG in Germany introduced stenbolone acetate in 1961. Approximately two years later, Syntex would introduce the drug to the United Kingdom, and soon after Mexico, under the brand name Anatrofin. Farmacologico Latino also sold this drug in Spain, under the generic name Stenbolone. It was reportedly applied (most commonly) as an injectable alternative to Anadrol in cases of Anemia, although little information about the clinical use of this agent survives today. The distribution of stenbolone acetate did not expand from its original markets, and ultimately enjoyed a relatively short lifespan as a pharmaceutical product. The last commercial preparation containing this ingredient was reportedly withdrawn from market (voluntarily) in the early 1980s. Its demise was likely financially driven, as Anatrofin disappeared at a time when many pharmaceutical manufacturers were dropping their lesser-used anabolic/androgenic steroids.
European bodybuilders were disappointed when Anatrofin was removed from the global market a couple of decades ago. Its loss was a hard felt one, very much like the old Primobolan acetate injectables. Old timers often claimed that the likes of this steroid were never replaced with the other popular non-aromatizable anabolics. Whether or not this is based on realistic experience or simple nostalgia remains to be seen. It is difficult today to say how different this agent ultimately is from methenolone or 1-testosterone, close chemical and pharmacological relatives which we have much more modern experience with. Until such time as this agent goes into wide-scale production again, which seems unlikely (at least as a prescription product), the true nature of stenbolone will remain elusive to the modern bodybuilding community. This steroid does, however, remain as an interesting chapter in the history of anabolic steroids.
How is Anatrofin Supplied
Stenbolone acetate is no longer available as a prescription drug product. When manufactured, it contained 25 mg, 50 mg, or 100 mg of steroid per milliliter of oil, packaged in 1 ml glass ampules.
Structural Characteristics of Anatrofin
Stenbolone is a derivative of dihydrotestosterone. It contains one additional double bond between carbons 1 and 2, and one additional methyl group at carbon 2, which helps to stabilize the 3-keto group and increase the steroid’s anabolic properties. Anatrofin makes use of stenbolone with a carboxylic acid ester (acetic acid) attached to the 17-beta hydroxyl group. Esterified steroids are less polar than free steroids, and are absorbed more slowly from the area of injection. Once in the bloodstream, the ester is removed to yield free (active) stenbolone. Esterified steroids are designed to prolong the window of therapeutic effect following administration, allowing for a less frequent injection schedule compared to injections of free (unesterified) steroid.
Anatrofin Side Effects (Estrogenic)
Stenbolone is not aromatized by the body, and is not measurably estrogenic. An anti-estrogen is not necessary when using this steroid, as gynecomastia should not be a concern even among sensitive individuals. Since estrogen is the usual culprit with water retention, this steroid instead produces a lean, quality look to the physique with no fear of excess subcutaneous fluid retention.This makes it a favorable steroid to use during cutting cycles, when water and fat retention are major concerns.
Anatrofin Side Effects (Androgenic)
Although classified as an anabolic steroid, androgenic side effects are still possible with this substance, particularly with higher than normal therapeutic doses. This may include bouts of oily skin, acne, and body/facial hair growth. Anabolic/androgenic steroids may also aggravate male pattern hair loss. Women are warned of the potential virilizing effects of anabolic/androgenic steroids. These may include a deepening of the voice, menstrual irregularities, changes in skin texture, facial hair growth, and clitoral enlargement. Stenbolone is a steroid with relatively low androgenic activity relative to its tissuebuilding actions, making the threshold for strong androgenic side effects comparably higher than with more androgenic agents such as testosterone, methandrostenolone, or fluoxymesterone. Note that stenbolone is unaffected by the 5-alpha reductase enzyme, so its relative androgenicity is not affected by the concurrent use of finasteride or dutasteride.
Anatrofin Side Effects (Hepatotoxicity)
Stenbolone is not a cl 7-alpha alkylated compound, and not known to have hepatotoxic effects. Liver toxicity is unlikely.
Anatrofin Side Effects (Cardiovascular)
Anabolic/androgenic steroids can have deleterious effects on serum cholesterol. This includes a tendency to reduce HDL (good) cholesterol values and increase LDL (bad) cholesterol values, which may shift the HDL to LDL balance in a direction that favors greater risk of arteriosclerosis. The relative impact of an anabolic/androgenic steroid on serum lipids is dependant on the dose, route of administration (oral vs. injectable), type of steroid (aromatizable or non-aromatizable), and level of resistance to hepatic metabolism. Stenbolone should have a stronger negative effect on the hepatic management of cholesterol than testosterone or nandrolone due to its non-aromatizable nature, but a much weaker impact than c-17 alpha alkylated steroids. Anabolic/androgenic steroids may also adversely affect blood pressure and triglycerides, reduce endothelial relaxation, and support left ventricular hypertrophy, all potentially increasing the risk of cardiovascular disease and myocardial infarction.
To help reduce cardiovascular strain it is advised to maintain an active cardiovascular exercise program and minimize the intake of saturated fats, cholesterol, and simple carbohydrates at all times during active AAS administration. Supplementing with fish oils (4 grams per day) and a natural cholesterol/antioxidant formula such as Lipid Stabil or a product with comparable ingredients is also recommended.
Anatrofin Side Effects (Testosterone Suppression)
All anabolic/androgenic steroids when taken in doses sufficient to promote muscle gain are expected to suppress endogenous testosterone production. Without the intervention of testosterone-stimulating substances, testosterone levels should return to normal within 1-4 months of drug secession. Note that prolonged hypogonadotrophic hypogonadism can develop secondary to steroid abuse, necessitating medical intervention.
Anatrofin Administration (Men)
The usual dosage among male athletes is in the range of 200-300 mg per week, taken for 8 to 12 weeks.This level of use is sufficient to notice moderate increases in strength and lean mass. Note that due to the short-acting nature of acetate esters, the weekly dosage is typically divided into three separate applications.
Anatrofin Administration (Women)
Female athletes would likely notice excellent gains and minimal virilizing activities on a dosage of 25-100 mg per week, taken in cycles no longer than 4 to 6 weeks. Note that due to the short acting nature of acetate esters, the weekly dosage is typically divided into two or three separate applications.
Anatrofin Availability
Stenbolone acetate is no longer manufactured as a prescription drug product.
References
Wlliam Llewellyn (2011) – Anabolics
Your experience with Anatrofin — stenbolone acetate
Anadur — nandrolone hexyloxyphenylpropionate
Andarine — S4, GTx-007

Winstrol (Stanozolol), What Does Winstrol Do
About Author
baxx
Doctor Baxx is an internationally recognized leader in the competitive bodybuilding industry. Its advanced bodybuilder and fitness training specialist certification provides beginners with opportunities for further advancing their knowledge and skills with bodybuilding at the advanced level.